This Is Me: Anwar’s Turning Point
“This is me. No more secrets. No more shame.” The words are simple. But for Anwar, they carry years behind them. Years of living with… Read More »This Is Me: Anwar’s Turning Point
“This is me. No more secrets. No more shame.” The words are simple. But for Anwar, they carry years behind them. Years of living with… Read More »This Is Me: Anwar’s Turning Point
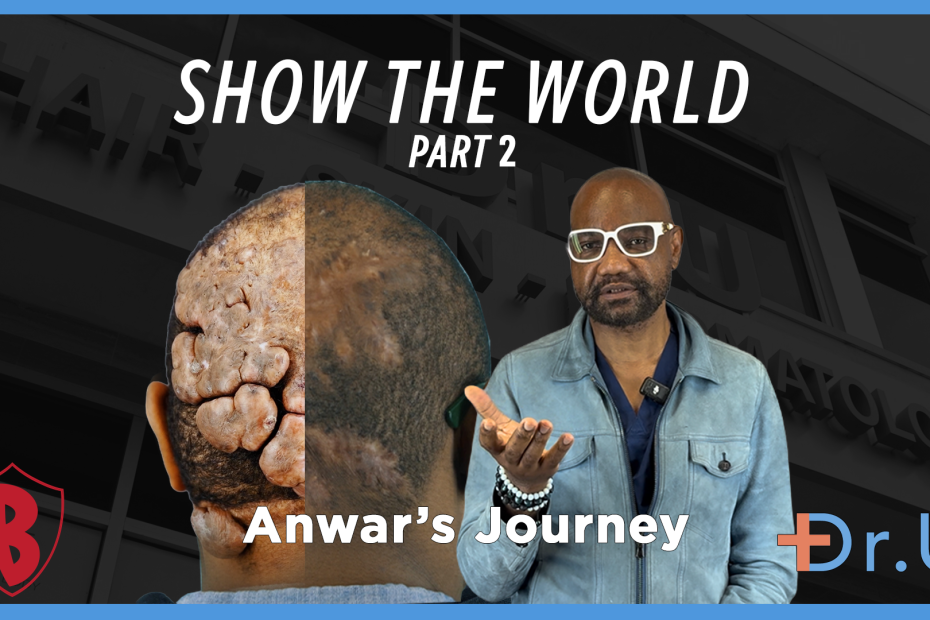
This moment feels different. Anwar steps into the room carrying something new. Not just energy from travel, not just calm in the air around him.… Read More »When Anwar Chose to Be Seen Again After Years with AKN
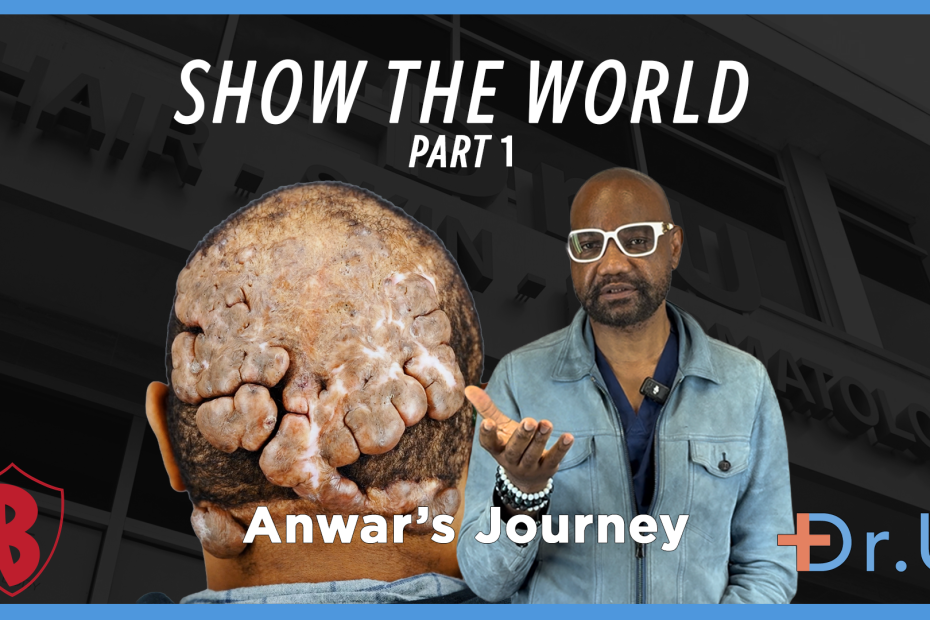
It is time. Not just a moment, but the end of years. Years of living with bumps on the back of the head. Years of… Read More »When Anwar Finally Took the Hat Off

For a long time, Anwar felt like he stood out. Not by choice. Not by personality. But because of something on the back of his… Read More »When Anwar Finally Blended Back Into Life After Years With AKN

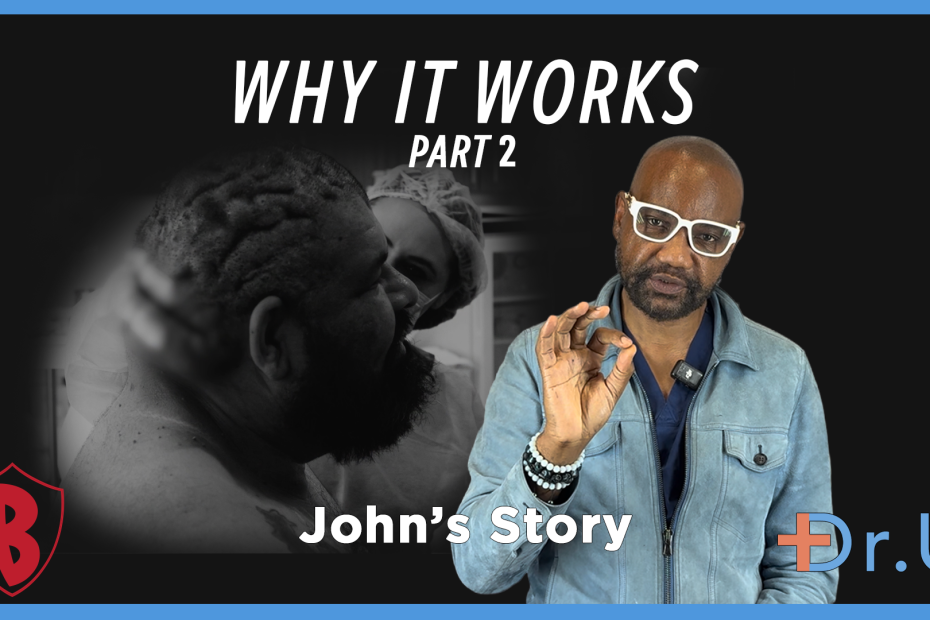
Before the surgery, John remembers what life felt like. Heavy. Not just on his scalp – but on his choices, his energy, his sense of… Read More »When Scalp Keloids Take Hold of Life
John’s scalp story did not begin with a dramatic moment. It began quietly. Small bumps appear along the back of the scalp. A little irritation… Read More »When Chronic Folliculitis of the Nape Starts the Inflammatory Chain

John’s journey began the way many scalp conditions do. With small bumps. At first, they appeared along the back of his head near the neckline.… Read More »When Two Scalp Diseases Collide: John’s AKN and Dissecting Cellulitis Story
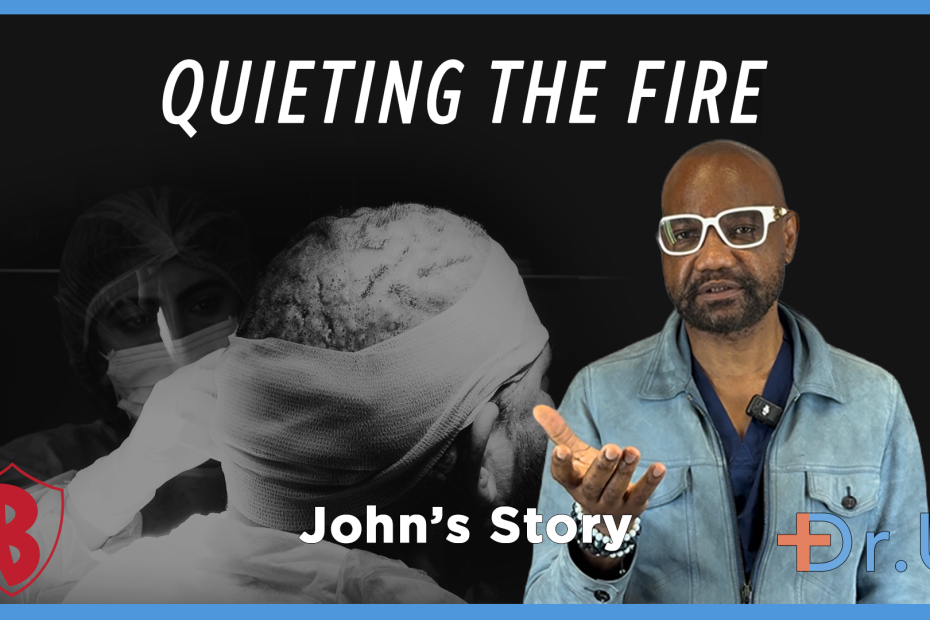
Pus bumps on the scalp treatment reached a turning point the day John’s surgery was completed. After hours of careful work, Dr. Sanusi Umar and… Read More »Quieting the Fire: Treating John’s Pus-Filled Scalp Bumps
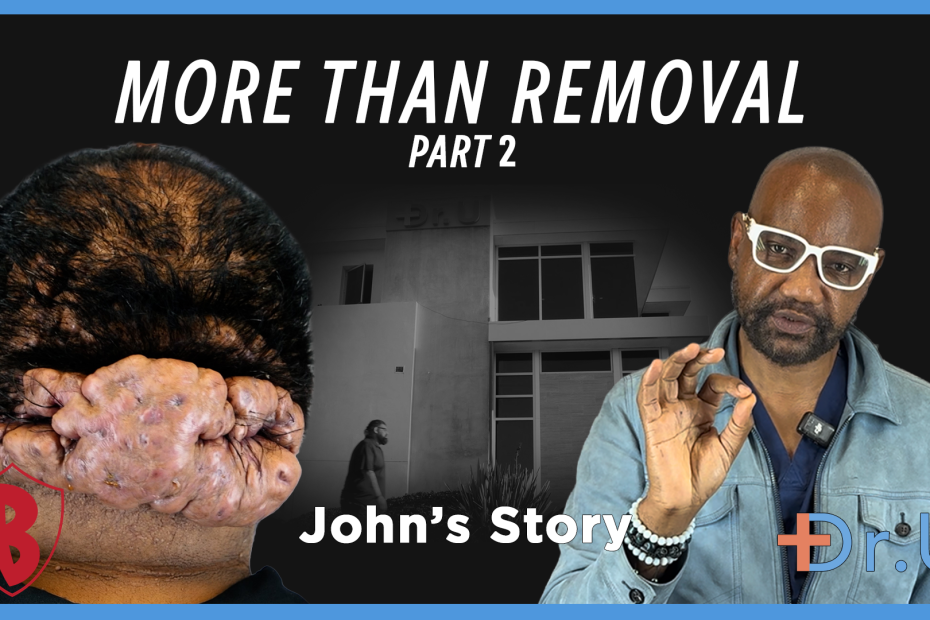
Posterior scalp scarring disorder treatment continued as the surgical team moved into the most critical phase of John’s procedure. Inside the operating room, Dr. Sanusi… Read More »Surgery That Goes Deeper: Treating John’s Posterior Scalp Scarring Disorder (Part 2)
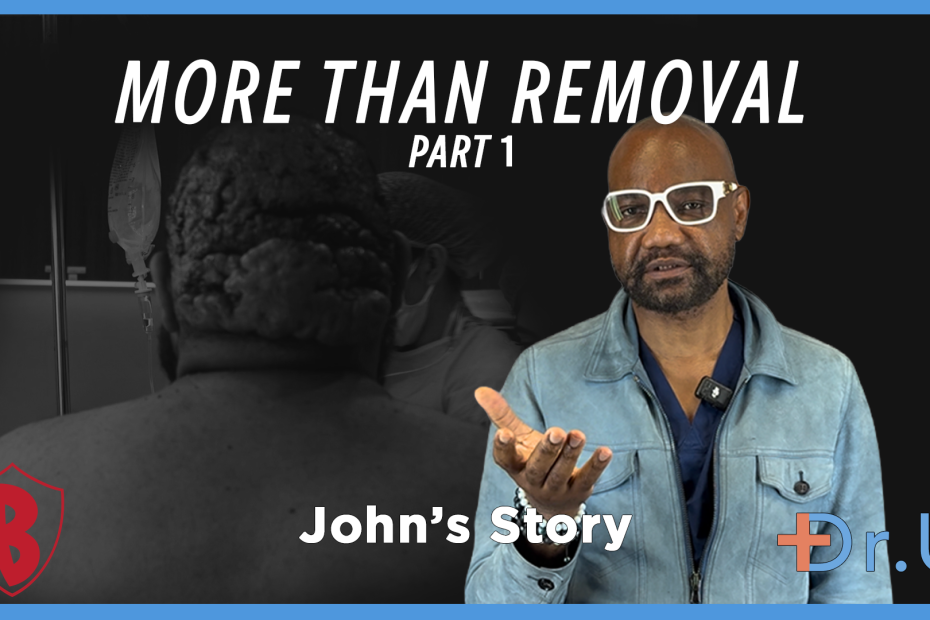
Posterior scalp scarring disorder treatment reached a defining moment today. It was John’s surgery day. Inside the clinic, the surgical team moved with calm focus.… Read More »More Than the Removal of Posterior Scalp Scarring Disorder (Part 1)
