Folliculitis Decalvans Treatment
Do You Want to Get a Permanent Solution to Your Folliculitis Decalvans (FD) Condition? Folliculitis Decalvans (FD) is a form of scarring Alopecia that is… Read More »Folliculitis Decalvans Treatment
Do You Want to Get a Permanent Solution to Your Folliculitis Decalvans (FD) Condition? Folliculitis Decalvans (FD) is a form of scarring Alopecia that is… Read More »Folliculitis Decalvans Treatment

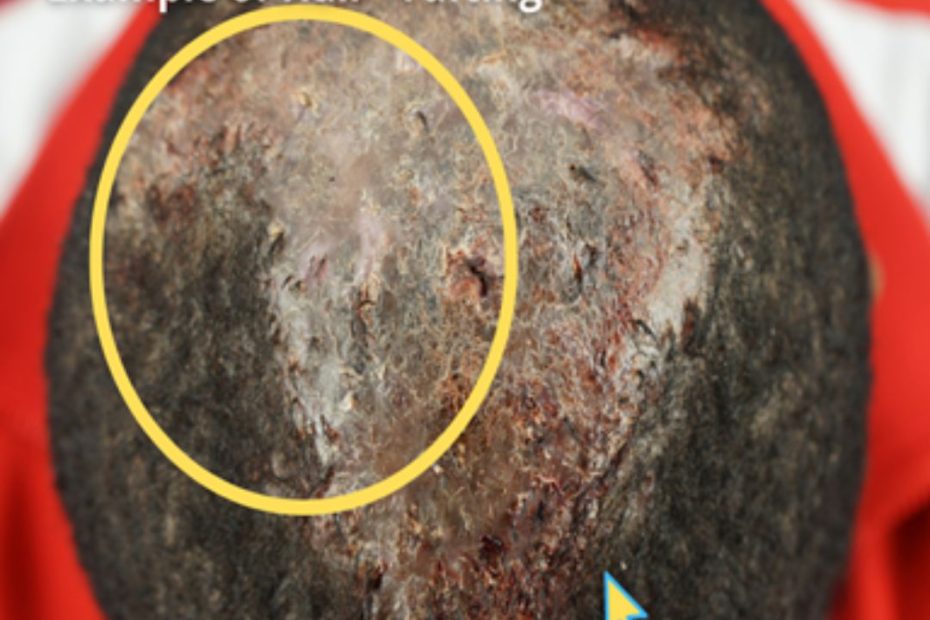
Dissecting Cellulitis (DC) is a long-term cicatricial (scarring) form of alopecia (hair loss) characterized by abscesses and keloids on the infected areas. This condition has… Read More »Dissecting Cellulitis Treatment
