When Anwar Finally Blended Back Into Life After Years With AKN
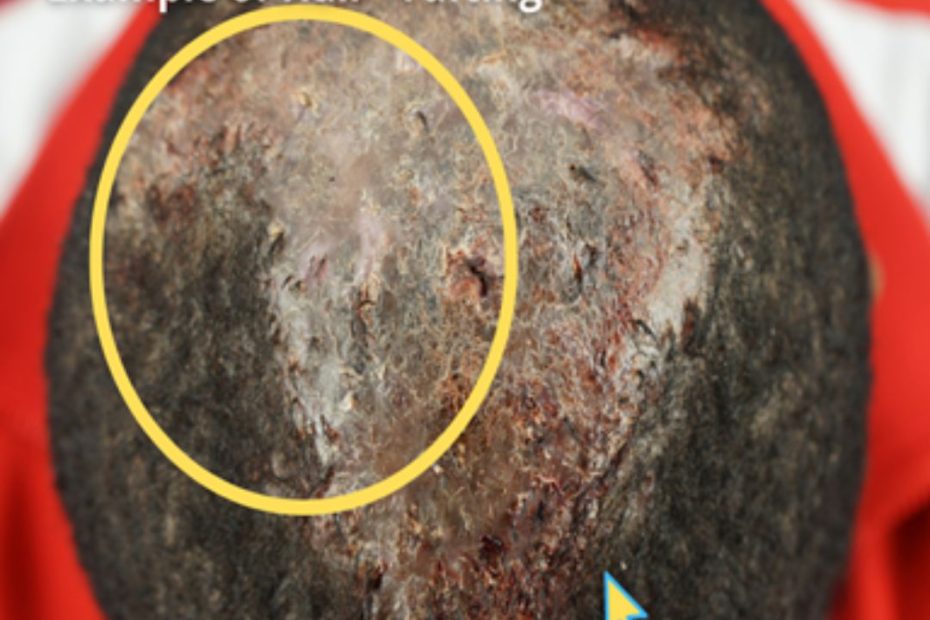
For a long time, Anwar felt like he stood out. Not by choice. Not by personality. But because of something on the back of his… Read More »When Anwar Finally Blended Back Into Life After Years With AKN